What happens when you combine a novel virus with an uninformed political decision making? You get an unprecedented, global economic calamity never witnessed in human history, one that will change the face of our current world unlike any other. With several billion people being forced into lockdown over the SARS CoV2 (COVID-19) pandemic, the world has just experienced one of the most disastrous polices in modern times.
Over the last 100 years there were three major pandemics; The “Spanish Flu,” 1918-1920, with an estimated 50 million fatalities worldwide; the “Asian Flu,” 1957-1958, with an estimated 1.5 million fatalities worldwide; and the “Hong Kong Flu,” 1968-1969, with around 1 million fatalities people worldwide. None of these pandemics required a global shutdown in the magnitude of what we are experiencing.
On an episode on Lockdown TV, the presenter was interviewing Professor Neil Ferguson from the Faculty of Medicine at the Imperial College London; the architect of the model which predicted over 2.2 million deaths in the US and over 500,000 in the UK from the pandemic. The presenter asked Ferguson if a model was also done to show the deleterious aspects of the lockdown and his response was no. In fact, Professor Ferguson and his team had already stated in another published paper on March 26th, ”we do not consider the wider social and economic costs of suppression, which will be high and may be disproportionately so in lower income settings”.
Essentially, Ferguson and Imperial College were admitting that a complimentary Cost Benefit Analysis (CBA), comparing lives versus lives, was not part of the decision making. This would suggest they were indirectly valuing the novel and unknown COVID-19 mortality and disregarding the known predictable mortalities. Their model’s assumption was based primarily on the virus’ basic reproductive number, the R0 value, which is the average number of people who will get the virus from someone who is infected. This model is what was ultimately presented to the world as a reason for the global lockdown.
A cost benefit analysis, however, is the process by which Ferguson and many of the world’s leading organizations could have analyzed the lockdown predetermination, identifying the benefits of its action, as well as the associated costs and thereby subtracting those costs from the benefits. At the end, the CBA would have provided results that could have been used to implement reasonable conclusions around the feasibility and advisability, of a lockdown decision. This strategy of a CBA is employed not just by profit making operations, but also by governments and non-profit entities. It is a foundational principle and tool, that I myself use as a Supply Chain Analyst. We use it when identifying the highest and best returns on our investments and our outcomes, based on resources, cost and most importantly, the risks involved.
In this article, we will attempt to provide you with what a CBA would have looked like in the eyes of those making the decisions to lockdown the entire planet, including the World Health Organization (WHO), the Center for Disease and Control in the US (CDC), The European Union (EU) and The National Health Services (NHS) of the Britain.


What led to the lockdown decision and what did we know?
On January 30th, we knew that the WHO Director-General Tedros Adhanom Ghebreyesus declared that the virus was an emergency which required international attention, noting the potential spread of the virus to countries with weak health systems. He also noted that the case fatality rate at that time was around 3.4 percent. A percentage based on the proportion of people who died from the disease concurrent with those diagnosed with COVID-19, over and up to that period of time.
On March 11th, theWHO declared the virus was now a pandemic and stated“we are deeply concerned both by the alarming levels of spread and severity and by the alarming levels of inaction,” adding that, “we have called every day for countries to take urgent and aggressive action.”
On March 24th, the WHO Collaborating Centre for Infectious Disease Modeling; MRC Centre for Global Infectious Disease Analysis, at the Imperial College London, came out with a model that predicted 40 million lives would be lost globally, 2.2 million people would die in the US and over 500,000 would die in the UK if no action was taken.
Following the WHO recommendations and the model from Imperial College, many leaders around the world, in perfect sequence, reacted with a somewhat draconian lockdown on or about March 26th. They told their nation’s citizens that this was a preventive measure to slow the spread of an extremely deadly and novel virus and to prevent the medical systems from being overwhelmed. Although the idea sounded laudable at the time, this entire decision was made primarily on the basis of a “highly speculated” model from Imperial College, a model which was developed without a complimentary Cost Benefit Analyst (CBA), comparing lives versus lives and also without the benefit of being peer reviewed by other academics.
However, there were some very brilliant minds who were analyzing the Imperial model and were suggesting that the decision to impose a lockdown was unnecessary and we should pursue an alternative course. John P. A. Ioannidis, a professor of medicine, epidemiology and biomedical data science at Stanford University, had computed the death rate at between 0.05 per cent and 1 per cent. Professor Ioannidis called the fatality rate of 3.4 per cent reported by the (WHO) “meaningless”.
We also had Professor Michael Levitt, a biophysicist and the 2013 Nobel laureate in chemistry, who analyzed the early data of cases worldwide and suggested that actions such as a lockdown or social disruptions were totally unnecessary and that the data did not support such actions. He said, what we needed to do “is control the panic” and in the grand scheme of things, “we are going to be fine”. His brilliance was on full display when he predicted at the end of February, the number of confirmed cases of COVID-19 in China would reach approximately 80,000 and the death toll 3,250. These numbers based on his predictions turned out to be almost 100% accurate by mid March.
One last thing we knew. In 2009, a government estimate based on the same Ferguson’s advice said, a “reasonable worst-case scenario” was that the swine flu would lead to 65,000 British deaths. In the end, swine flu killed 457 people in the U.K, a far cry from his estimate.
I gave those facts because I believe context matters, especially when some people are still defending the lockdown measures and are suggesting that we didn’t know what to do at the time and that somehow, more lives would have been lost had we not done a lockdown. I say to those people, yes we did have enough information. There wasn’t then and there isn’t now, any logical evidence which can support the lockdown. In fact, all the evidence is pointing to the fact that there is no significant virus spread mitigation from the lockdown.
A new report and comprehensive mathematical study done by The Woods Hole Oceanic Institute, shows that the lockdown had little to no effect on the virus spread. They indicated that “the growth rates and reproduction numbers two to three weeks before the full lockdown policies would be expected to have visible effects”, however, this was not the case. The study went on to say that, a “comparison of pre and post lockdown observations reveals a counter-intuitive slowdown in the decay of the epidemic after lockdown. Estimates of daily and total deaths numbers using pre-lockdown trends suggest that no lives were saved by this strategy, in comparison with pre-lockdown, less restrictive, social distancing policies”.
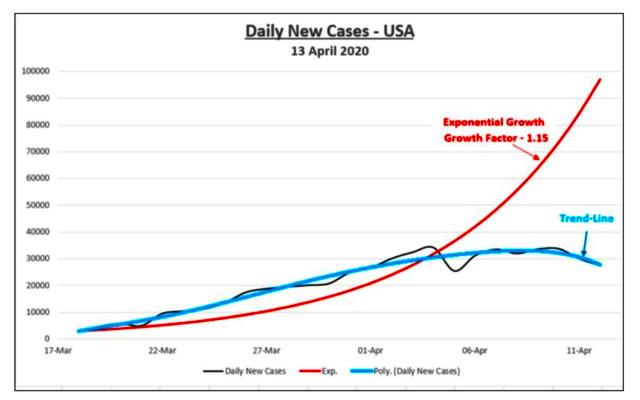
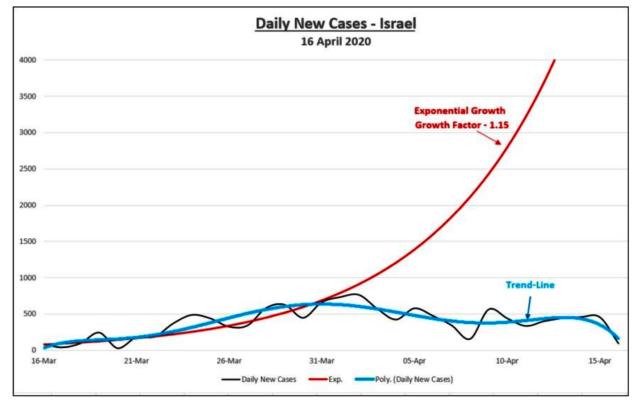
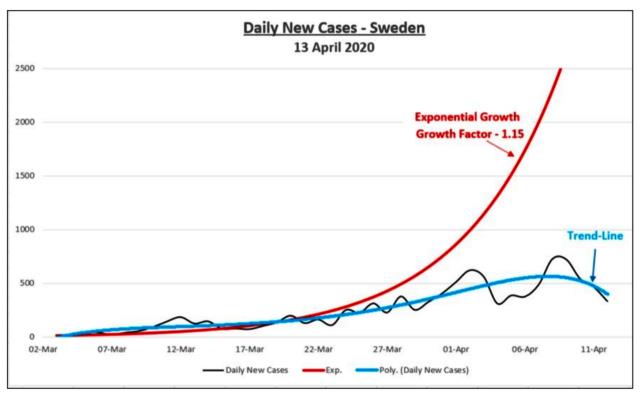
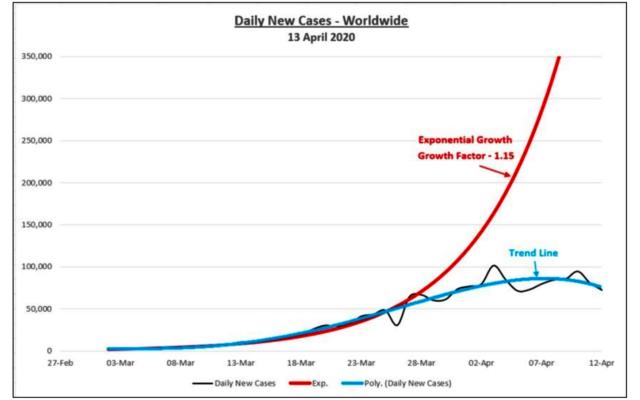
We also have Isaac Ben-Israel, a prominent mathematician, chairman of Israel’s Space Agency, who did a similar study and arrived at the same conclusion as the Woods study. His analysis found that the exponential growth and decline of COVID-19 showed a “constant pattern across countries”. He stated that “surprisingly, this pattern is common to countries that have taken a severe lockdown, including the paralysis of the economy, as well as to countries that implemented a far more lenient policy and have continued in ordinary life”.
The following charts from Professor Ben-Israel show the global comparison and the remarkably similar phenomenon, common to almost every country on the globe. Whether implementing full lock-down or no lockdown, as in the case of Sweden, the results are amazingly identical.
Considered some of the key facts leading up to the lockdown, these are some of the questions which would have been asked from a COVID-19 CBA perspective.
- Are we confident that the COVID-19 denominator is accurately represented?
- Have we ever quarantined healthy people to protect the vulnerable?
- How deadly were the previous strains of the Corona viruses?
- What was the average age profile of those that were dying out of the early numbers ?
- What is the age profile represented out of the Chinese numbers?
- What measures were taken to mitigate substantial deaths in China?
- How feasible was it to replicate the Chinese mitigation model in other countries?
- When was the last recorded lockdown in modern times?
- What are the opinions and consensus from renowned experts?
- Is this the deadliest virus we have ever faced based on the current data?
- How many lives will be lost in the short, medium and long term, as a result of the lockdown?
As mentioned previously, cost benefit analysis is a foundational principle, which offers unique and valuable insight and would have been useful in:
- Developing benchmarks for proposing a global lockdown
- Deciding whether to pursue a proposed lockdown
- Weighing decisional opportunities
- Measuring social benefits
- Appraising the desirability of suggested policies
- Assessing change initiatives
- Performing a sensitivity analysis (also known as a “what-if”)
- Quantifying effects on stakeholders and participants globally
- Having a well developed plan for post lockdown
There is really no “standard” format used when engaging a CBA, however, there are certain core elements that would have had to be present in this crisis, including:
- Deciding on a repeatable framework to outline the parameters of the analysis
- Identify costs and benefits so they can be categorized by type and intent
- Calculate costs and benefits across the assumed life of the pandemic
- Compare costs and benefits using aggregate information
- Analyze results and make an informed, final recommendation
The above process would have indeed provided a thorough step by step progression of all inputs in a very comprehensive way, whether direct or indirect and not in the interest of time and reduced the analytical process from over assumptions or guesses. Below we will go through a few of these elements in some detail.
Establishing a Framework for COVID-19
In establishing the framework for a COVID-19 CBA, firstly, the proposed program or policy change needed to be outlined in detail. This would have meant, looking carefully at exactly what was being evaluated in relationship to the problem being solved. For example, the analysis associated with the question, “should we recommend a global lockdown?” should have only been made, once a situational overview had carefully mapped the existing state of the virus around the world, starting with Wuhan, the suspected origin. This would have included but not limited to background data on historical global lockdown examples but also current performance, ie., the lockdown in Wuhan and other Chinese provinces. It would have also included any opportunities brought to the table and its projected performance in the future. Also, a real clear and an objective look at any risks involved in maintaining a non-lockdown scenario moving forward.
The next approach in this framework evaluation process would be to decide on how to approach cost, i.e, which cost/benefits should be included in the analysis. This would have included the obvious predictable negative implications like untreated illnesses, economics, social and moral implications among other factors, all measurable using historical analysis. One could also analyze the unforeseen future costs that could impact the initiative in both the short and long term.
With CBA, it is important to understand that in some cases, geography could play a role in determining feasibility of a project or initiative. Therefore a one size fit all approach is not always advisable, as stakeholders in different locales would be affected by the decision being analyzed. For example, the lockdown would clearly be a luxury for the middle and upper-classes especially in developed countries like Sweden, Switzerland, Germany, Canada, USA, etc. Conversely, it would be an absolute liability of enormous proportions in developing countries in the Caribbean, Africa and a country like India. In that case, it is important to make sure this is included into the framework upfront, so that unwanted negative effects can be identified and mitigated.
Identify and Categorize Costs and Benefits
After establishing the framework, sorting the costs and benefits into categories could have been the next step. These categories are direct/indirect, tangible/intangible and real and of course the ultimate benefit, saving lives.
- Direct costs-Direct medical costs include the cost of a defined intervention and all follow-up costs for other medication and health care interventions in ambulatory, in-patient, and nursing care
- Indirect costs- are usually fixed in nature and may come from a hospital’s overhead or cost center. The expenses incurred from the cessation or reduction of work productivity as a result of the morbidity and mortality associated with COVID-19. Indirect costs typically consist of work loss, worker replacement and reduced productivity
- Tangible costs- are measurable and quantifiable and are related to an increase in hospital beds, quarantine facilities, increased medical personnel, increased deficits due to unemployment costs, global economic downturn, inward supply chains, de-globalization, depression and recession
- Intangible costs-are difficult to identify and measure, such as shifts in regular patient treatment quality and productivity levels, the social disruption of people’s everyday lives, enjoyment and constitutional rights. Increased pain and suffering to millions worldwide
- Real costs-The number of lives which will potentially be lost due to the shutdown, i.e, from hunger, untreated cancers and heart disease and suicide are expenses associated with producing a global lockdown offering
Once the above categories have been established, it is time to start crunching the numbers as unbiased and unpolitical as possible. For the purpose of this exercise where the primary evaluation is human lives, the cost benefit factor would be limited to lives versus lives. Having established a framework and the important representative categories, a reasonable outlining of the overall costs and benefits would have followed. Again, it’s important that both short and long term considerations are factored in, so that projections are based on the life of the program and the evolution of both costs and benefits post lockdown.
COVID-19 Costs Assumptions-Deaths from Hunger
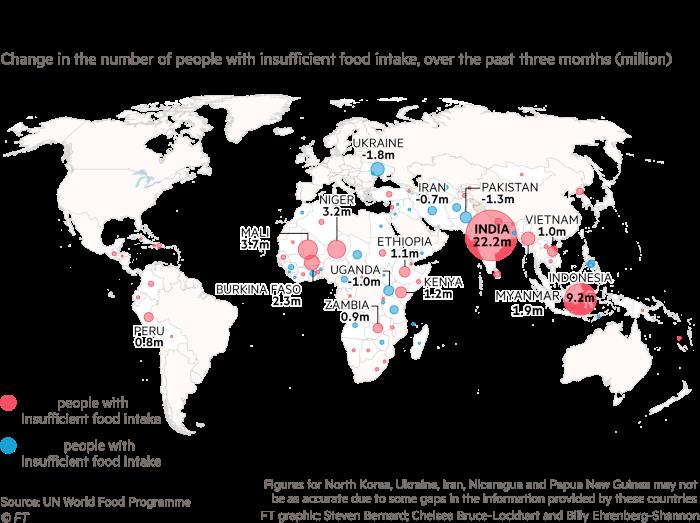
According to the WHO, 38 million people die each year from hunger and this has been on the rise in many countries where the economy has slowed down or contracted. Between 2011 and 2017, this increase coincided with an economic slowdown or downturn in 65 out of 77 countries. Furthermore, economic shocks tend to be significant secondary and tertiary drivers that prolong and worsen the severity of food crises, especially in countries experiencing acute food insecurity requiring urgent humanitarian assistance.

Global economic slowdowns and downturns like what we are facing, “often lead to a rise in unemployment and a decline in wages and incomes, challenging access to food and essential social services for the poor. People’s access to high-quality, nutritious food can be affected, as can access to basic services such as health care”. At a time when the UN is estimating the number of people suffering from hunger could go from 135 million to more than 250 million in the next few months, many of these are likely to be in east Africa, the Caribbean, India and other developing countries.
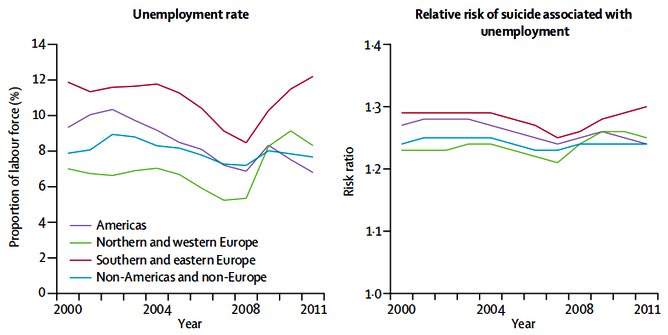
COVID-19 Costs Assumptions-Deaths from Suicide Due to Unemployment
Researchers have found that there had been an increase in the relative risk of suicide associated with unemployment, 20% to 30%across all regions. There were an estimated 233,000 suicides a year between 2000-11, of which around 45,000 could be attributed to unemployment. In 2007, the year before the crash, there were 41,148 identified cases of suicide. In 2009, this number had risen to 46,131 – an increase of 4,983 or 12%. Therefore if we look at the current economic situation which is several times greater and we use a conservative increased factor of 10, we would therefore arrive at a 120% increase in suicides from the lockdown. We believe that this would have been very conservative based on the fact that some US hotlines have reported an increase of 600% in calls during the lockdown.
COVID-19 Costs Assumptions-Deaths from Untreated Predictable Negatives
Another unintended but predictable negative from this global lockdown are the lives which will be lost due to missed healthcare treatment. This includes but not limited to, cancer treatments, organ transplantations, dialysis treatments, heart attacks and heart disease diagnosis and more. According to the American Institute of Economic Research, this could lead to approximately 46,000 lives for each month of the lockdown in the US alone.
The executive director and head of a global partnership to end tuberculosis (TB) Lucica Ditiu, said she is “sickened” by research that revealed millions more people are expected to contract the disease as a result of Covid-19 restrictions. She went on to say that “the fact that we’ve rolled back to 2013 figures and we have so many people dying, this for me is sickening”. “I am outraged that just by not being able to control what we do and forgetting about programs that exist we lose so much, starting with the loss of the lives of people.”
According to the Guardian newspaper, up to 6.3 million more people are predicted to develop TB between now and 2025 and 1.4 million more people are expected to die as cases go undiagnosed and untreated during lockdown. This will set back global efforts to end TB by five to eight years.
COVID-19 Costs and Benefits Analysis Calculations
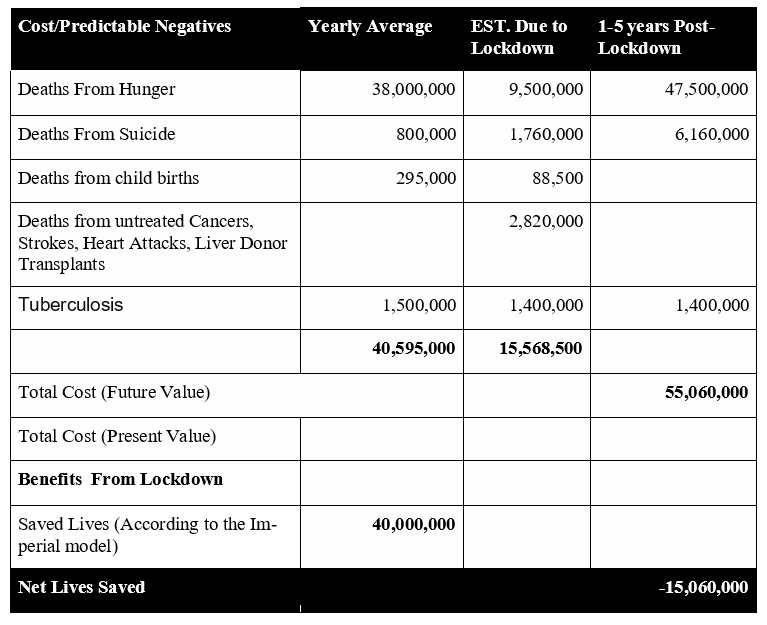
Costs or predictable negatives are based on historical data and projected rates of increase using conservative ratios; projected deaths from COVID-19 are based on projected models from Imperial College London.
- Deaths from hunger uses a ratio of 25% increase based on yearly average
- Deaths from suicide uses factor of 120% based on the magnitude of joblessness and associated data
- Deaths from child births uses a ratio of 30% from year average
- Deaths from untreated illnesses and procedures are based on the US prediction multiplied by 20 for a worldwide aggregate
- Tuberculosis numbers are based on data from TB foundation and Guardian report
- Deaths from hunger year 1-5 assumes that hunger will keep pace for the next 5 years due to the severity of food shortages from the lockdown
- Deaths from suicide in year 1-5 assumes a 30% reduction on the increase numbers per year after 2020, projecting a gradual reduction in unemployment globally
Here is the SANITY CHECK. If we accepted the model from the Imperial College, we can see by our calculation that the loss of lives superseded the lives saved. Therefore any reasonable and objective analyst would have said “no way, no how” to any lockdown suggestion. To date, the total mortality from COVID-19 stands at 381,000 according to Worldometer. When we multiply this number even by a factor of 5 to represent the next 5 years, we are actually projecting a net loss of 53,155,000 (55,060,000-1,905,000) lives.
In conclusion, models should never be applied and used as the basis for future global decision making and most certainly shouldn’t be presented without a comprehensive and supporting CBA. They can be useful tools for guiding policy, but they are only as credible as their assumptions. There is no doubt that the lockdown was an unmitigated disaster and it is therefore time for those who made the decision to admit it. If a CBA was done and the values remotely resembled what we have shown, then the decision to recommend a global lockdown would have been a resounding NO.
Precious lives will be lost now and for years to come due to these actions and we need some level of mea culpa from leaders. The fact existed then and it exists now, that some of the world’s most populous countries, home to well over 3 billion people, suffer extreme poverty under normal circumstances. Therefore the consequences of a lockdown would fuel extraordinary suffering and devastation which will last for generations. We now know based on the data we have seen, that firstly, the mortality rate is enormously less than what was first suggested. Secondly, the the mathematical models consistently agree that in all countries, the infection period started months prior to the lockdowns; therefore, this action had little positive effects. Finally, the deaths which will occur due to the lowdown decisions, will exceed that of COVID19 mortalities, exponentially. So, was the lockdown really worth it?
Written by Colan Caesar, co-founder of ICPM and a political marketing strategist
References:
Canary Foundation- Earl Detections Facts and Figures https://www.canaryfoundation.org/wp-content/uploads/EarlyDetectionFactSheet.pdf
Jenny Lei Ravelo, Sara Jerving- devex-https://www.devex.com/news/covid-19-a-timeline-of-the-coron- avirus-outbreak-96396
The Guardian-Millions predicted to develop tuberculosis as result of Covid-19 lockdown https://www.theguardian.com/global-development/2020/may/06/millions-develop-tuberculosis-tb-covid-19-lockdown
Imperial College London- Report 12 – The global impact of COVID-19 and strategies for mitigation and suppression- https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-12-global-impact-covid-19/
The Effect of Wait Times on Mortality in canada- https://www.fraserinstitute.org/sites/default/files/effect-of-wait-times-on-mortality-in-canada.pdf
Walter Muruet, MSc, Anthony Rudd, MD, Charles D.A. Wolfe, MD, and Abdel Douiri, PhDLong-Term Survival After Intravenous Thrombolysis for Ischemic Stroke-A Propensity Score-Matched Cohort With up to 10-Year Follow-Up- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5839705/
Jeffrey A. Tucker- https://www.aier.org/article/will-the-politicians-admit-their-lockdown-mistake/
World Health Organization- Suicide rates per 100 000 population – https://www.who.int/gho/mental_health/suicide_rates/en/
Woods Hole Oceanographic Institution, Falmouth, Massachusetts-Full lockdown policies in Western Eu- rope countries have no evident impacts on the COVID-19 epidemic. https://www.medrxiv.org/content/10.1101/2020.04.24.20078717v1.full.pdf
Isaac Ben-Israel-The end of exponential growth: The decline in the spread of coronavirus https://www.timesofisrael.com/the-end-of-exponential-growth-the-decline-in-the-spread-of-coronavirus/
American Institute for Economic Research-Will the Politicians Admit Their Lockdown Mistake? https://www.aier.org/article/will-the-politicians-admit-their-lockdown-mistake/
Eutostat- Standardised death rates for preventable diseases conditions, persons aged less than 75 years, 2016 (per 100 000 inhabitants) https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Standardised_death_rates_for_preventable_diseases_conditions,_persons_aged_less_than_75_years,_2016_(per_100_000_inhabitants)_HLTH19.png
Stop TB Partnership- The Global Plan to End TB 2018-2022 http://www.stoptb.org/global/plan/plan1822.asp
Merchant. M (2020)-When lockdowns become counter-productive- https://www.dailyo.in/variety/ covid-19-coronavirus-pandemic-lockdown-4-0-economic-impact-of-coronavirus-mental-health/story/ 1/32993.html
World Health Organization: WHO; available on: https://www.who.int/mental_health/prevention/suicide/suicideprevent/en/
UNFPA: United Nations Population Fund-Deaths from child births; available on: https://www.unfpa.org/maternal-health
Tuberculosis: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
4 Comments
mellisa · 25. August, 2020 at 3:56
A excellent article about covid 19, I just given this onto a colleague who was doing a analysis on this. And he ordered me lunch because I found it for him :). So let me rephrase that: Thankx for taking the time to talk about this, I feel strongly about it and enjoy learning more on this topic. If possible, as you become expertise, would you mind updating your blog with more info? It is extremely helpful for me.
Kelci Jerrie · 26. August, 2020 at 3:33
Bonjour, toujours super de voir d’autres personnes à travers le monde du trou dans ma recherche, j’apprécie vraiment le temps qu’il aurait fallu pour créer cet article génial. À votre santé Kelci Jerrie Knitter
debora · 30. August, 2020 at 19:38
Ich habe Ihren Artikel mit Interesse gelesen.
Janice Darbee Leif
Gerda · 9. December, 2020 at 2:25
Way cool! Some extremely valid points about the virus! I appreciate you penning this post and the rest of the website is also very good. Gerda Basilio Marijo